Christine Fekete, PhD1,2, Beat Gurtner, MSc1, Simon Kunz, PhD1,2, Armin Gemperli, PhD1,2, Hans Peter Gmünder, MD3, Margret Hund-Georgiadis, MD, PhD4, Xavier Jordan, MD5, Martin Schubert, MD, PhD6, Jivko Stoyanov, PhD, EMBA1 and Gerold Stucki, MD, MS1,2,7, for the SwiSCI Study Group

From the 1Swiss Paraplegic Research, Nottwil, 2Department of Health Sciences and Medicine, University of Lucerne, 3Swiss Paraplegic Center, Nottwil, 4REHAB Basel, Basel, 5Clinique Romande de Réadaptation, Sion, 6Paraplegic Center University Clinic Balgrist, Zurich, 7Center for Rehabilitation in Global Health Systems, WHO Collaborating Center, Department of Health Sciences & Medicine, University of Lucerne, Switzerland
Objectives: To provide a methodological reference paper for the inception cohort of the Swiss Spinal Cord Injury Cohort Study (SwiSCI), by detailing its methodological features and reporting on participant characteristics, response rates and non-response bias.
Design: Prospective cohort study starting in 2013 in all 4 specialized rehabilitation centres in Switzerland. Subjects: Included are 655 newly diagnosed first rehabilitation patients aged ≥16 years with traumatic or non-traumatic spinal cord injury (TSCI, NTSCI).
Methods: Descriptive statistics were used to depict participant characteristics and to compare characteristics of responders and non-responders. Logistic regressions were conducted to estimate non- response bias.
Results: The sample consisted of 69% males, with mean age 53.5 years, 57.9% TSCI, 60.7% paraplegia and 78.8% incomplete SCI. Males and younger persons more often sustained TSCI and more severe SCI, resulting in longer duration of rehabilitation. Complete lesions were more prevalent in TSCI compared to NTSCI. The response rate was 47.5% and study participation was less likely in females, older persons, persons with lower functional independence and those with NTSCI.
Conclusion: SwiSCI inception cohort data enable the estimation of epidemiological figures of SCI in Switzerland, and prognostic and trajectory modelling of outcomes after SCI to guide policy, service provision and clinical practice.
Key words: inception cohort; spinal cord injury; first rehabilitation; cohort profile; non-response bias; SwiSCI; biobank.
Accepted Jan 22, 2021; Epub ahead of print Feb 11, 2021
J Rehabil Med 2021; 53: jrm00159
Correspondence address: Christine Fekete, Guido A. Zäch Strasse 4, 6207 Nottwil, Switzerland. E-mail: christine.fekete@paraplegie.ch
Doi: 10.2340/16501977-2795
The inception cohort of the Swiss Spinal Cord Injury Cohort Study (SwiSCI) is a prospective study including newly diagnosed first rehabilitation patients aged over 16 years with traumatic or non-traumatic spinal cord injury (SCI) who received first rehabilitation in a specialized center in Switzerland. This paper describes the methods and the design of the SwiSCI inception cohort and reports on participant characteristics, response rates and differences between respondents and non-respondents. The response rate was 47.5% and 655 patients participated in the study. Of participants, 69.0% were male, mean age was 53.5 years, 57.9% had traumatic SCI, 60.7% paraplegia and 78.8% incomplete SCI. Male subjects and younger persons more often sustained traumatic SCI and more severe SCI, resulting in longer duration of rehabilitation. Complete lesions were more prevalent in traumatic SCI compared with non-traumatic SCI. Females, older persons, persons with lower functional independence and those with non-traumatic SCI were less likely to participate in the study.
Inception cohorts are prospective studies including a designated group of people assembled at a common time-point near the onset (“inception”) of symptoms, early after diagnosis, or at detection of a pathological event (1). Although these studies are time and cost-intense, inception cohorts offer substantial added value to research and practice, as they have considerable methodological strengths. Given that the time after exposure at which patients begin their prospective follow-up assessments is standardized, inception cohort data offer the opportunity to investigate relationships between early or acute post-exposure factors and long-term outcomes or different patient trajectories after onset of an event (2, 3). Inception cohort data may also enable the investigation of relationships among risk factors, treatments and outcomes, and therefore provide valuable observational evidence to inform the development and implementation of randomized controlled trials (RCTs) (4, 5). As cohort studies in the community setting are particularly prone to mortality bias, inception cohorts present valuable designs to estimate key epidemiological figures, such as incidence rates of specific conditions (3). Moreover, if data collection is performed in direct contact with participants, data quality issues, such as recall bias and missing data can be minimized.
The inception cohort of the Swiss Spinal Cord Injury Cohort Study (SwiSCI) is a prospective observational cohort study that collects a wide-range of demographic, biopsychosocial, clinical parameters and biological samples from persons newly diagnosed with traumatic or non-traumatic spinal cord injury (TSCI, NTSCI), who are receiving specialized first rehabilitation in Switzerland (6). The SwiSCI inception cohort aims to provide a high-quality scientific evidence-base for the comprehensive study of functioning, health maintenance, subjective well-being and survival after SCI. Given that SCI is a life-altering condition with a sudden onset, which requires specialized inpatient rehabilitation, the sensitive phase early after injury and the related first rehabilitation often has a critical impact on the long-term development of health conditions, functioning and well-being (7–9). The sudden onset of an SCI also requires substantial psychological adaptation and puts newly injured persons at increased risk of reduced mental health, including depression and anxiety disorders (10, 11). Insights into the trajectories of health, functioning, and well-being during inpatient rehabilitation and early after reintegration into community, as well as prognosis for health-related outcomes after SCI may help to guide intervention planning and decision-making in health professionals, service providers and patients to optimize the situation of persons with SCI in the long-term (12).
In summary, the SwiSCI inception cohort is a research platform that provides a sound basis to estimate key epidemiological figures regarding SCI in Switzerland (i.e. incidence, all-cause and cause-specific mortality) and to build prognostic models on health, functioning and well-being over the life course of people with SCI to guide policy, service provision and clinical practice. This reference paper aims to provide a comprehensive description of the methodological features of the SwiSCI inception cohort, to describe participant characteristics, response rates and potential non-response bias in the data collected between May 2013 and September 2020.
Design
Data are prospectively collected at 4 measurement time-points (T1–T4) during first inpatient rehabilitation in 4 specialized SCI rehabilitation centres in Switzerland (6). T1–T3 follow fixed time-windows, scheduled in relation to weeks after SCI diagnosis (weeks 4, 12 and 24) and T4 is assessed at time of discharge from first rehabilitation. T5 is scheduled one year after SCI diagnosis, and mostly takes place after discharge during the routine check-up closest to 1 year after diagnosis, when most participants live in the community (Fig. 1). As this schedule is not applicable to all participants, given the considerable variations in length of first rehabilitation, the schedule is adapted if discharge T4 is before T1, T2 or T3. To compensate for the lack of complete sets of measurement time-points in participants with adapted assessment schedules, adapted measures (i.e. questionnaires including items that are part of questionnaires from later measurement time-points) are used to collect most important information from missed measurement time-points. Participants completing T5 are subsequently followed up in the SwiSCI community survey, which takes place every 5 years (6, 13). Data collection in the inpatient setting started by 1 May 2013, and in the outpatient setting by 1 August 2016. Biobank sampling (at T1 and T4), started on 27 June 2016 in the largest centre (Nottwil), followed by 2 other centres (Basel and Sion) on 23 August 2018 and 15 January 2019. This paper reports on data collected in the inpatient setting during the period 1 May 2013 to 1 September 2020. Fig. 1 provides an overview of the foreseen and effective assessment schedule. Approximately one-third of participants followed the planned assessment schedule with no overlaps, while assessments overlapped in approximately two-thirds of participants.
Fig. 1. Assessment schedule of the Swiss Spinal Cord Injury Cohort Study (SwiSCI) inception cohort: study protocol vs effective schedule. SCI: spinal cord injury. T1: measurement time-point at admission. T2: measurement time-point 12 weeks after diagnosis. T3: measurement time-point 24 weeks after diagnosis. T4: measurement time-point at discharge. T5: measurement time-point 1 year after diagnosis.
Governance and ethics
All 4 major SCI rehabilitation centres in Switzerland (SCI Center of Balgrist University Hospital, Zurich-Balgrist; Centre for SCI and Severe Head Injury of REHAB Basel, Basel, Clinique Romande de Réadaptation, Sion; Swiss Paraplegic Centre, Nottwil) contribute to this inception cohort. The SwiSCI Study Center, located at Swiss Paraplegic Research, Nottwil, is responsible for the planning and operational conduct of the study. Trained research assistants are in charge of recruitment and data collection in the centres, and bi-annual meetings with the Study Center are held to optimize data quality and standardization of procedures. Data quality measures and workflows are described in formally approved standard operational procedures. Details of the SwiSCI governance structure are reported elsewhere (6). The SwiSCI biobank is certified by the Swiss Biobanking Platform (https://swissbiobanking.ch) for governance, ethics and legal compliance and standard operational procedures.
Responsible regional ethics committees (documents EKNZ 100/13, LU 12090; KEK Zurich 2013-0249; CE Valais 032/13) approved the study protocol and all assessments. Regulations concerning informed consent and data protection are strictly observed and informed consent is mandatory for study participation.
Sample
The SwiSCI inception cohort recruits Swiss residents aged over 16 years who are newly diagnosed with TSCI or NTSCI and are admitted for first rehabilitation into 1 of the 4 specialized rehabilitation centres. Excluded from the study are persons with congenital conditions leading to SCI, including spina bifida, new SCI in the context of palliative care, neurodegenerative disorders including multiple sclerosis and amyotrophic lateral sclerosis, and Guillain-Barré syndrome.
Fig. 2 provides an overview on the consent scenarios and the possible participation status of eligible individuals, which are indicated in yellow circles: (1) non-response with denial of any data use, (2) non-response with no consent to SwiSCI, but general consent to use clinical routine data (minimal data-set; MDS), (3) participation with collection of full data-set (FDS; 3a: with blood-sampling, 3b: without blood-sampling), (4) participation with collection of FDS plus separate informed consent for collection and storage of bio-samples in the SwiSCI biobank for generalized use in future scientific projects, undergoing further ethics evaluation. Likewise, additional informed consent is needed for the data collection at measurement time-point T5 in the outpatient setting.
Fig. 2. Flow chart of consent scenarios and participation status. FDS: Full data set. MDS: Minimal data set.
Recruitment
After eligibility screening, research assistants approach patients newly admitted for first rehabilitation to explain the study and provide written information and informed consent forms. As patients may be incapable of deciding about participation in the sensitive early stage after injury, patients are approached as soon as responsible clinicians consider personal contact adequate. In case patients are unable to consent due to acute cognitive impairment, their legal representative is asked for general consent to use clinical routine data for research purposes. Research assistants are kept informed about the patient’s capacity of discernment and patients who have regained capacity receive study information and are asked for consent personally later on. If consent is obtained after T1, T2 or T3, research assistants retrospectively collect available information for the elapsed time-points from the medical records. In adolescents younger than 18 years, parental consent is needed for participation. No data are collected in case of chronic cognitive impairment or if persons are discharged before consent is obtained.
Data model
Any data in the inpatient setting T1–T4 are collected by extraction of routine data from the medical records, by clinical assessments, and by paper-and-pencil questionnaires. At T5, data are collected by clinical assessments, questionnaires and computer-assisted telephone interviews. Questionnaires and interviews are available in German, French, Italian and English.
The data model of the SwiSCI inception cohort is based on the International Classification of Functioning, Disability and Health (ICF), with the Brief ICF Core Sets for SCI in the early post-acute context as reference for the clinical setting (14) and the Brief ICF Core Sets for SCI in the long-term setting as reference for the community setting (15). Brief ICF Core Sets were developed to guarantee that the most important dimensions of functioning and contextual factors are systematically evaluated in clinical practice and research. The identification of relevant psychological and personal factors was based on a systematic review proposing 7 categories to be assessed in SCI research (16). Given the clinical context of the study, a wide spectrum of routinely collected data on health conditions, body functions and structures are also included in the data model. The selection of measures to operationalize the data model was based mainly on feasibility and comparability criteria. An inventory on routinely used measures in the collaborating centres was elaborated and established measures were prioritized and harmonized across the 4 centres. Furthermore, the “International SCI Basic Data Sets” suggested by the International Spinal Cord Injury Society (https://www.iscos.org.uk/international-sci-data-sets) were prioritized whenever appropriate and available. Data additionally collected to the routine data mainly concerns the self-report data on personal and psychological factors. The selection of measures was based on a systematic process, described elsewhere (17). Importantly, measures that were previously used in the SwiSCI community survey were preferred in order to allow comparisons. Within the framework of the SwiSCI biobank, a minimally invasive collection of the primary biological specimens, blood and urine, allows the effective processing and cryopreservation of high-quality RNA, DNA, immune cells (peripheral blood mononuclear cells), serum, plasma, urine supernatant and urine sediment. An overview of the data collected in the SwiSCI inception cohort is shown in Table SI.
Data and sample management
Data are continuously entered into a password-secured web-based SQL database, and recruitment outcomes can be monitored in real time. For security reasons, only research assistants and dedicated personnel from the SwiSCI Study Center can access data. Personal data of participants is stored separately from research data (pseudonymized). Participants are assigned with a unique identifier, and personal as well as research data contain the unique identifier (SwiSCI ID). Data storage, validation, monitoring, update, and backups are performed centrally at the SwiSCI Study Center following standardized procedures. Biosample handling is performed only with encrypted samples, which are transferred for processing and cryopreservation the SwiSCI biobank according to validated workflows and standard operational procedures. Researchers can apply for SwiSCI inception cohort data and samples by submitting a research proposal to the Study Center (swisci.research@paraplegie.ch) that undergoes an internal peer review process. Upon approval of the research proposal, pseudonymized data are provided to researchers for analysis. Samples for analysis are provided after an additional approval by the responsible ethics committee.
Measures
Information on sex, age at injury (in years), neurological level of injury, SCI severity based on grades of the American Spinal Injury Association Impairment Scale (AIS) (18), aetiology of injury, length of stay in first rehabilitation (in days), functional independence and depressive symptoms in early and late stages of first rehabilitation was used to describe the sample. AIS grades from the measurement time-point T1 (4 weeks after injury), or in case of missing AIS at T1, the available information from subsequent time-points, T2, T3 or T4, were used. Injury levels C1–C8 were classified as tetraplegia, and levels at and below T1 as paraplegia. Injury severity (complete, incomplete) was determined based on information on AIS grades, whereby grades A were coded as complete and all others as incomplete injury. A 4-category variable combining level and severity of injury was created for analysis (paraplegia complete, paraplegia incomplete, tetraplegia complete, tetraplegia incomplete). Functional independence in activities of daily living was measured with the Spinal Cord Independence Measure (SCIM) III, comprising 19 items on the grade of independence in daily tasks, which are rated by health professionals and weighted according to their clinical relevance (19, 20). The SCIM-III total score ranges from 0 to 100, with higher scores indicating higher functional independence (20). Depressive symptoms were assessed with the depression subscale of the Hospital Anxiety and Depression Scale (HADS-D) (21). The HADS-D comprises 7 4-point scaled items on common symptoms of depressive disorders in the past week. A sum score ranging from 0 to 21 was calculated, with higher scores indicating more depressive symptoms, and scores ≥ 8 indicating a severity of depressive symptoms that is of clinical concern (22).
Statistical analysis
Statistical analyses were performed using Stata version 16.0 (College Station, TX, USA). Frequency statistics were used to describe recruitment outcomes and basic characteristics of participants, whereby the number of persons and percentages (%) were indicated for categorical variables, and means, and standard deviations (SD), medians and interquartile ranges (IQR) were indicated for continuous variables. Stratified descriptions of basic participant characteristics were provided by aetiology, SCI level and severity, and rehabilitation centre. χ2 tests were used to compare dichotomous or categorical variables in the subgroups. Due to the non-normal distribution of included continuous variables, Kruskal–Wallis tests were used to compare the distribution of continuous variables in the corresponding subgroups.
For the assessment of potential non-response bias, basic characteristics from non-respondents (for whom the minimal data-set was available) were compared with participant characteristics. For categorical variables, cross-tabulations and p-values from χ2 tests were calculated and for continuous variables, means were compared with Kruskal–Wallis tests and corresponding p-values are reported. Furthermore, consent status (participation vs non-response) was regressed on sex, age at SCI, SCI level and severity, aetiology, SCIM-III scores at admission, and rehabilitation centre. Logistic regressions were used and all predictors were simultaneously included in the model to predict participation. AIS scores were not included in models due to high collinearity with the combined variable on SCI level and severity and HADS-D scores were unavailable for non-responders. Odds ratios (OR), 95% confidence intervals (95% CI) and p-values from likelihood ratio tests are shown in results Table II and Table III. All analyses are based on complete cases and the number of missing values is reported in the respective tables. Of note, only 12 participants who initially consented to the full data-set withdrew their consent during the course of the study and given this small number no additional non-response analysis was performed to assess bias due to attrition.
Study aim 1: Description of participant characteristics
Basic sociodemographic and lesion characteristics of the total sample, stratified by aetiology, SCI lesion and severity, and rehabilitation centre are shown in Table I. Approximately 70% of participants were male, TSCI was more prevalent than NTSCI (57.9% vs 42.1%), incomplete paraplegia was the most frequent diagnosis (43.8%), and complete tetraplegia the least frequent (5.0%). Mean age at injury was 53.5 years and participants spent a mean of 140 days in first rehabilitation. Approximately, 41% of participants were treated in centre 1 (Nottwil), 26% in centre 2 (Balgrist) and approximately16% in centres 3 and 4 (Sion and Basel, respectively).
TSCI was more prevalent in males and younger age groups, more often resulted in complete lesions, and participants with TSCI underwent a mean of 48 days longer first rehabilitation than those with NTSCI. Complete lesions and tetraplegia were more often observed among males, younger persons and were associated with longer duration of first rehabilitation.
SCIM-III and HADS-D scores were more favourable at discharge discharge than at admission, indicating that functional independence increased and depressive symptoms decreased from admission to discharge. Mean SCIM-III scores at admission were lower for participants with TSCI than those with NTSCI (36.4 vs 48.9), but differences at discharge were no longer significant (68.7 vs 72.3). SCIM-III scores varied according to SCI level severity, with lowest scores in complete tetraplegia (11.0 at admission, 31.4 at discharge) and highest in incomplete paraplegia (48.8 at admission, 77.4 at discharge). Mean HADS-D scores were generally higher at admission than at discharge, with mean scores being below the cut-off, indicating a clinically relevant severity of depressive symptoms (i.e. > 8) at both time-points, except for persons with complete tetraplegia at admission. Persons with complete lesions generally reported higher HADS-D scores than those with incomplete lesions; however, differences were more pronounced at admission than at discharge.
Basic characteristics of participants varied markedly across rehabilitation centres. Differences were observed between centres in terms of sex and age distributions (23–44% females; mean age 50–58 years), and in terms of lesion characteristics (tetraplegia 35–53%; complete lesions 11–28%, TSCI 47–68%), length of stay (98–179 days), and indicators of functioning (SCIM-III at admission 34.7–48.0, HADS-D at admission 4.8–7.5, at discharge 3.9–6.2). However, there were no significant differences in SCIM-III scores across centres at discharge.
Study aim 2: Assessment of response rates and potential non-response bias
The overall response rate for the period of May 2013 to September 2020 is 47.5%, indicating the percentage of participants related to the total of eligible patients. For the biobank starting recruitment later, a total of 407 persons were eligible. Of the eligibles, 206 refused participation, 201 participated in SwiSCI and of those participants, 106 additionally consented to the biobank. Response rates for the biobank were therefore 26.0% in relation to the total eligible population and 52.7% in relation to the participant-population.
Table II shows the basic characteristics of participants and those non-responders for whom minimal data were available. The distribution of sex, SCI level and severity, and aetiology was similar between both groups, whereas age at SCI and SCIM-III scores varied in the sense that participants were generally younger and had higher functional independence than non-respondents. Males, younger persons and persons with TSCI more often consented to the biobank than did females, older persons and persons with NTSCI, while the SCI level and severity or functional independence measured by SCIM-III were not related to biobank participation. Participation rates for general participation and additional participation in the biobank varied considerably between centres.
Results from regression modelling on study participation are shown in Table III. Males, younger persons, persons with TSCI and higher SCIM-III scores were more likely to participate in the SwiSCI inception cohort. Likewise, younger persons and males were more likely to additionally consent to the biobank, while aetiology was no longer a predictor for participation in biobanking in the multivariable model.
Table I. Basic characteristics of the 655 contemporary Swiss Spinal Cord Injury Cohort Study (SwiSCI) inception cohort participants, stratified by aetiology, spinal cord injury (SCI) severity, and rehabilitation centre
Table II. Comparison of basic characteristics of non-responders and participants of the Swiss Spinal Cord Injury Cohort Study (SwiSCI) inception cohort
Table III. Prediction of participation by basic sociodemographic and lesion characteristics: Results from logistic regressions showing odds ratios (OR) and 95% confidence intervals (95% CI) for participation
This paper provides a methodological reference for research based on SwiSCI inception cohort data, which is prospectively collected among persons with newly acquired SCI in Switzerland. A total of 47.5% of eligible patients participated in the study, and the sample is characterized by a predominance of males (70%), mean age of 53.5 years, higher rates of TSCI (57.9%), paraplegia (59.5%) and incomplete injuries (79.3%). Different demographic profiles and length of first rehabilitation were observed according to lesion characteristics: TSCI was more prevalent in males and younger patients, and more often resulted in complete lesions and longer duration of first rehabilitation. Similarly, males and younger persons often sustained more severe SCI than did females and older persons, resulting in longer duration of rehabilitation. However, the study sample might not be fully representative of incident cases of SCI in Switzerland, as older persons, females, persons with lower functional independence and those with NTSCI were more likely to refuse to participate in the study. Also, females and older patients more often refused to participate in the SwiSCI biobank.
Participant characteristics
Patterns of key characteristics in the current sample reflect well-known characteristics of newly injured persons with SCI. For example, the higher prevalence of males in SCI populations is well established and, especially for TSCI, mainly explained by the higher risk exposure related to the work environment and preferences in leisure, sports and transportation use (23–36). Mean age at injury was 49 years for TSCI and 59 years for NTSCI in the current study cohort, which is comparable to the mean age of newly injured adults reported elsewhere in Europe (Sweden TSCI 55 years (25); Norway TSCI/NTSCI 49/52 years (26); Netherlands TSCI/NTSCI 43/57 years (28)). While there is good evidence showing that the proportion of NTSCI has increased over the past decades due to population ageing, the prevalence of TSCI varies widely between studies, ranging from approximately 38% (31) to 75% (23, 32). Although prevalence comparisons are difficult, the distribution according to basic characteristics observed in the current sample is fully in line with current evidence indicating that TSCI is more prevalent in males and younger age groups (28, 31–36) and results in more severe lesions than NTSCI (26, 31–33, 35). The age trend is mainly due to the fact that TSCI is often work-related, and thus more prevalent in the employable age group (32), and that younger people are typically more involved in potentially risky sports, leisure and transport-related activities (25, 36). Also, it is not surprising that males and younger persons often have more severe SCI in the current study sample, as the physical forces causing SCI differ by aetiology. Low-level falls and NTSCI often observed among elderly people result in less severe or incomplete lesions compared with the more frequent high-level falls, traffic or work accidents, where much stronger forces come into play (25, 36).
The longer duration of first rehabilitation in TSCI compared with NTSCI patients detected in the current sample has been reported previously (26, 28, 31, 32) and is mainly due to more severe injuries in TSCI, the fact that the trauma itself often causes additional injuries (e.g. fractures, abdominal injuries) and the higher prevalence of medical complications during first rehabilitation in TSCI (32, 37). Congruent to earlier findings reporting higher functional impairment in TSCI compared with NTSCI (26, 31–33, 35) and the finding that TSCI patients tend to have a larger reduction in impairments between admission and discharge (31), the current study observed generally lower SCIM-III scores for TSCI than NTSCI at admission, but higher improvement for the TSCI group at discharge. This might be due to the higher mean age in NTSCI, underlying aetiological reasons, and shorter first rehabilitation (32). The finding that HADS-D scores in the current study were generally higher at admission than at discharge may indicate that rehabilitative activities and time since onset support psychological adaptation. However, this view on mean scores is rather simplistic, neglecting variability in individual trajectories of psychological adaptation after SCI (11). Furthermore, substantial variation in basic characteristics of participants according to rehabilitation centre were observed in this Swiss setting, highlighting the importance of running inception cohorts with a multi-centre approach, as missing out one of the centres might result in biased samples, given that patients with specific profiles would be systematically excluded.
Potential non-response bias
The results of the current study indicate that older persons, females, persons with lower functional independence and those with NTSCI are less likely to participate in the inception cohort, and females and older persons were less likely to consent to the SwiSCI biobank. We speculate that the lower participation of females and persons with lower functional independence is due to higher preoccupation with physical challenges and the adaptation process in this sensitive phase early after injury, reducing the readiness to accept other commitments, such as participation in research. As reported for the SwiSCI inception cohort, males and patients with higher functional independence showed more favourable psychological adaptation profiles (11), probably influencing resources to participate in research. However, it was not possible to validate this assumption, as information on psychological adaptation was unavailable for non-responders. As one-fifth of non-respondents rejected any use of data and was therefore excluded from non-response analysis, it is important to note that the evaluation of the extent of bias remains imprecise. Moreover, given that data collection is ongoing, non-response patterns are not a fixed property and need to be reassessed whenever new participants are enrolled. As non-response bias can seriously affect the generalizability of findings (38, 39), the calculation of updated non-response patterns and the development of inverse probability weights to correct for the underrepresentation of patients with specific characteristics is recommended to account for potential bias (39). It is difficult to make a general statement on the extent of non-response bias affecting study results, however, as it varies depending on the variables of interest. Sensitivity analysis comparing weighted and unweighted results can help to identify the extent of bias.
In addition to refusal to participate in the study, item non-response presents another methodological challenge. While the problem of missing values is lower for data that is collected in clinical routine (except if measurement time-points overlap, as shown in Fig. 1), the additional data collected via questionnaires present higher susceptibility to missing values, as participants might actively refuse to respond to questionnaires or are in a poor health status impeding the collection of non-routinely assessed data at a given time-point. A substantial number of missing values are, for example, detected in the HADS-D, with approximately 29% and 23% missing values at admission and discharge, respectively. These high rates of missing data need detailed analysis on whether the complete cases are a completely random subsample of the total sample in relation to relevant variables (i.e. missing completely at random; MCAR) or not. If the subsample of complete cases are not MCAR, complete case analysis can lead to substantial information loss, but also to considerable risk for biased inferences. A description and analysis of the structure of missing data in relation to basic respondent characteristics and the imputation of missing values are considered appropriate strategies to increase the validity of findings (39, 40). The comparison between complete case analysis and analysis based on imputed values may further help to assess the robustness of findings.
Study limitations
Although the 4 specialized SCI rehabilitation centres in Switzerland were included in the recruitment of participants, it must be acknowledged that the generalizability to the target population of incident cases of SCI in Switzerland may be restricted. First, patients with SCI were missed if they received first rehabilitation in a non-specialized, neurological rehabilitation centre, as might be the case for patients with lower SCI severity and older age. Secondly, data of persons who died in the acute setting before they could be admitted to any of the 4 specialized centres were missed and, therefore, mortality bias in the study sample cannot be excluded. Thirdly, 11% of eligible patients refused the use of their data, thus limiting the validity of our non-response analysis. Since this is a prospective study with ongoing data collection, non-response patterns are dynamic and need to be re-examined whenever new patients are enrolled. Weighting analysis, using inverse probability weights, can be a valuable tool to reduce bias. Item non-response in non-routinely collected data presents another methodological challenge that requires the use of multiple imputation techniques to reduce bias.
Conclusion
The SwiSCI inception cohort presents a rich database that allows to estimate key epidemiological figures on SCI for Switzerland, to build prognostic models and trajectories of health, functioning and subjective well-being after the onset of SCI to guide policy, service provision and clinical practice. Although certain patient groups were slightly underrepresented in the current study sample, well-established demographic profiles and length of rehabilitation according to lesion characteristics, were observed.
The authors thank the SwiSCI Steering Committee with its members Xavier Jordan, Fabienne Reynard (Clinique Romande de Réadaptation, Sion); Michael Baumberger, Hans Peter Gmünder (Swiss Paraplegic Center, Nottwil); Armin Curt, Martin Schubert (University Clinic Balgrist, Zürich); Margret Hund-Georgiadis, Kerstin Hug (REHAB Basel, Basel); Laurent Prince (Swiss Paraplegic Association, Nottwil); Heidi Hanselmann (Swiss Paraplegic Foundation, Nottwil); Daniel Joggi (Representative of persons with SCI); Nadja Münzel (Parahelp, Nottwil); Mirjam Brach, Gerold Stucki (Swiss Paraplegic Research, Nottwil); and Armin Gemperli (SwiSCI Coordination Group at Swiss Paraplegic Research, Nottwil).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize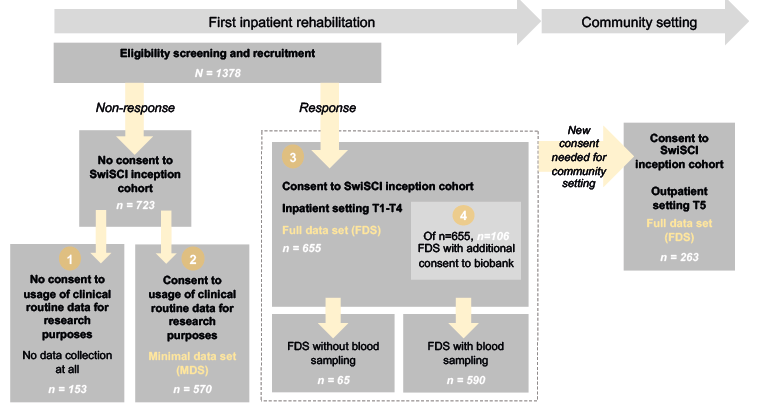 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize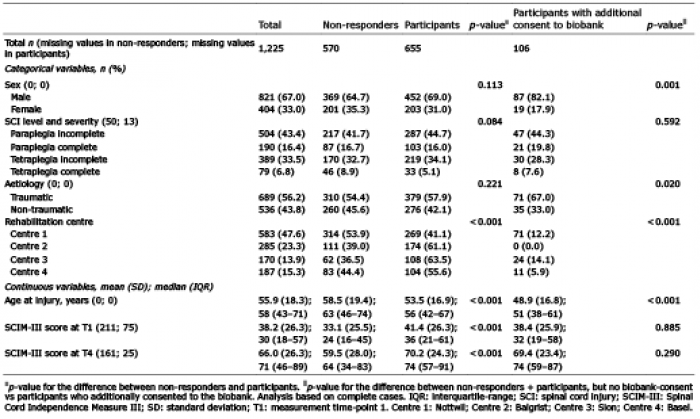 Click to show fullsize
Click to show fullsize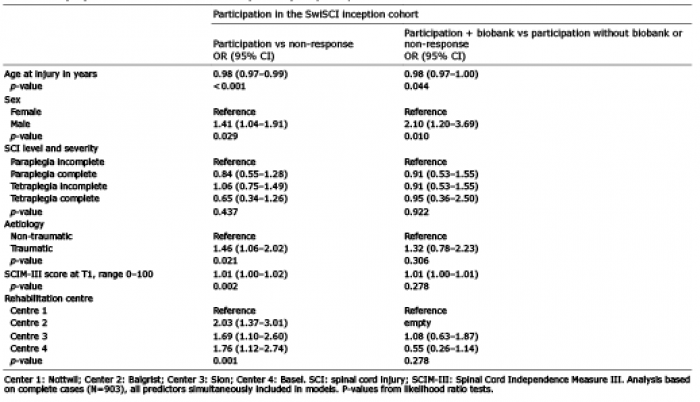 Click to show fullsize
Click to show fullsize